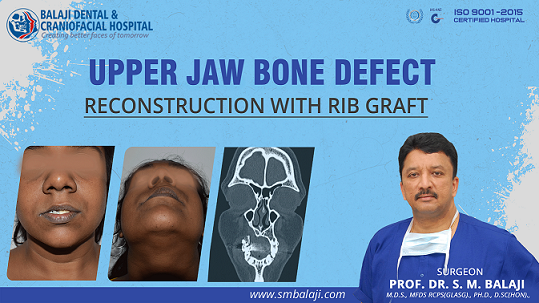
Patient develops a swelling in the region of the maxillary right anterior teeth
The patient is a 24-year-old female from Nanguneri in Tamil Nadu, India. Over a period of two years, she had begun to notice a slow growing swelling in the maxillary right incisor region. Since there had been no pain or discharge associated with it, she had ignored it for a long time. It was firm to the touch and not painful.
Some of her neighbors soon began commenting on the subtle change in her facial structure. It was only then that she decided to seek medical opinion for her upper jaw bone defect. Her parents had been referred to a nearby city hospital by some well wishers.
A biopsy had been obtained by the oral surgeon, which revealed a diagnosis of benign ossifying fibroma. He explained that this needed to be excised. Teeth in the involved region would be extracted. Artificial teeth would be placed once the surgical site had healed. The patient was particular that she did not want a removable denture.
What is a benign ossifying fibroma and what are its causes
This arises from the periodontal ligament and can be considered to be a benign neoplasm. There is expansion of the overlying cortical plates. Perforation of the overlying structures is never seen due to the slow growing nature of the lesion. Differential diagnosis includes reactive hyperplasia
Surgical excision of the benign ossifying fibroma from the maxillary bone
The patient underwent excision of the lesion along with extraction of the overlying right central and lateral incisors and the right canine. After a period to allow for complete healing of the surgical wound, the patient was referred to a prosthodontist. Rehabilitation was completed by constructing a bridge to replace the three extracted teeth.
The patient however was not happy with her postoperative appearance. She felt that her right alar base and lips had a sunken appearance. There was also food impaction in the region above the bridge, which was causing halitosis. The patient desired correction of her complaints.
She therefore presented with a general surgeon who obtained imaging studies. Seeing that the bony defect was very large, he counseled her to approach an expert oral and maxillofacial surgeon. The patient made enquiries and was referred to our hospital for management.
Patient presents at our hospital for initial consultation for her bony defect
Dr SM Balaji, jaw reconstruction specialist, examined the patient and obtained imaging studies. This revealed that the patient had a defect of around 14 mm. He explained to the patient that rib grafts needed to be harvested for filling in the jaw defect. This would be followed by placement of dental implants to complete rehabilitation for the patient.
Successful reconstruction of the jaw defect using rib grafts harvested from the patient
Under general anesthesia, an inframammary incision was made and rib grafts were harvested. A Valsalva maneuver was then performed to ensure that there was no perforation into the chest cavity.
Attention was next turned to the region of the maxillary bony defect. A mucogingivoperiosteal flap was raised to expose the defect. The rib bone graft was then crafted to perfectly fit into the bony defect.
These were then fixed in place with titanium screws. Hemostasis was checked and the flap was closed with sutures.
Patient instructed to return in four months for dental implant surgery
Bony consolidation of the grafts to the surrounding alveolar bone would take up to four months. The patient was therefore instructed to return after four months for dental implant surgery. She expressed understanding of the instructions and thanked the surgical team before discharge from the hospital.
Patient with chronic tooth infections in his maxillary anterior teeth
The patient is a 28-year-old male from Pune in Maharashtra, India. He is an entrepreneur with his own startup company. Around 12 years ago, he had been injured while playing hockey in school. This had resulted in the fracture of his maxillary central incisors, left lateral incisor and left canine.
He had undergone root canal treatment of the four teeth along with bridge fixation. This had however turned into a chronic problem for the patient. He regularly developed pain and swelling in the region. This had been a constant source of discomfort for the patient.
Multiple apicoectomy procedures had been performed over the years for the involved teeth. This had however not provided long term resolution of his symptoms. His teeth had also become mobile due to bone loss from recurrent infections to the area.
Social difficulties arising from his long standing dental problem
The patient has also had long standing problems with food impaction and resultant halitosis. This had gotten to the point that it began affecting his work. He then decided to seek a permanent solution to this long standing problem.
The patient had visited a dental clinic where imaging studies had been obtained. The dental professional had also conducted a thorough intraoral examination.
This had revealed highly mobile teeth along with extensive alveolar bone loss and gum disease. Periodontal ligament attachment had been destroyed. There was also a periapical cyst in relation to the affected region.
The patient was informed that he needed treatment from an experienced oral and maxillofacial surgeon for his problems. He was then referred to our hospital for treatment. Oral and maxillofacial surgery in a cutting edge superspecialty at our hospital.
The patient had subsequently researched our hospital over the Internet. He made further enquiries using his professional contacts in Chennai. Having finally satisfied himself about the quality of services, he had contacted our hospital manager and made an appointment.
Initial consultation at our hospital to address his long standing dental difficulties
Dr SM Balaji, bone graft dental implant specialist, examined the patient and obtained imaging studies. This revealed that the patient had root canal treated upper central incisors and left lateral incisor and canine. There was extensive alveolar bone resorption of the involved area. This had resulted in grade 2 anterior mobility of the involved teeth.
It was explained to the patient that it was just a matter of time before the teeth were lost. He was advised upper jaw reconstruction with bone grafts. This would be followed by fixing of implants to the rib grafts. Final step of rehabilitation would involve fabrication of a bridge to replace the missing anterior teeth.
This was explained to the patient in detail and he consented to undergo surgery.
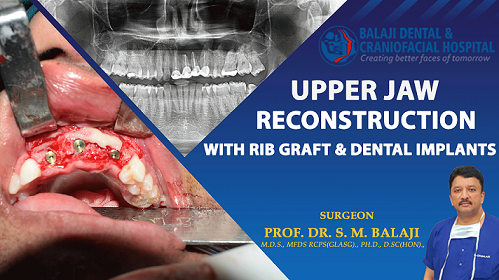
Successful placement of rib grafts along with dental implants in the maxillary anterior region
Under general anesthesia, a mucogingivoperiosteal flap was first raised over the region of the involved teeth. The four involved teeth were extracted and the cystic lesion was removed in its entirety. Friable infected bony tissue was then removed with a bur.
Attention was then turned to harvesting the bone graft. An inframammary incision was made followed by harvesting of a rib graft. This was followed by a Valsalva maneuver to ensure that there was no perforation into the thoracic cavity. The incision was then closed in layers with sutures.
The bone graft was then crafted to fit perfectly into the region of bony defect in the anterior maxillary region. This was then fixed in position with titanium screws. The patient was instructed to return in four months for fixation of implants in the bone grafts.
It would take a period of four months for complete bony consolidation of the grafts with the surrounding alveolar bone.
Patient returns in four months for placement of dental implants
The patient returned after a period of four months for dental implant surgery.Three Nobel Biocare dental implants were fixed in the consolidated bone grafts. The patient was instructed to return after four months for placement of a dental bridge.
He reported back as instructed after osseointegration of the implants to the alveolar bone. A Ceramic bridge was then fabricated to complete the rehabilitation process for the patient.
The patient was very satisfied with the results of his treatment. He said that he could not even differentiate between his natural teeth and the ceramic bridge. The patient thanked the entire team before final discharge from the hospital.
The patient involved in a head-on car crash while on a work trip
The patient is a 26-year-old businessman from Pune in Maharashtra, India. About a year ago, he had driven down to a nearby city for work. While there, he was involved in a head on collision with another automobile. His head had impacted directly on the steering wheel resulting in extensive lower facial injury. He had not been wearing his seatbelt at the time of the accident.
He suffered a fractured lower jaw along with fractured teeth in both jaws. An ambulance had been summoned and he was immediately shifted to a nearby hospital. Imaging studies obtained at the hospital revealed bilateral body of the mandible fractures near the premolar region. He had also suffered fractures to maxillary and mandibular anterior teeth.
There were no injuries to his eye sockets and bone fractures to other facial structures. This type of injury is very common to unrestrained drivers. They can be life threatening and surgeons with special training are required to address these complex injuries.
Complications of malunion and infection with resultant loss of alveolar bone
An emergency surgery had been performed and his bilateral mandibular fractures had been stabilized with titanium plates. His fractured anterior teeth were also extracted.
Within a month after surgery, it became evident that the surgery had been poorly performed. Bilateral fracture fixation sites developed an infection. This resulted in extensive resorption of the anterior alveolar bone. The height of the alveolus was greatly reduced.
Referral to our hospital for management of complications of previous surgery
The patient presented at a local hospital for management of his problem. Imaging studies were obtained. The patient was informed that he had suffered from extensive alveolar bone loss secondary to the infection.
There was malunion of the fracture repair with infected plates. Postsurgical suturing had been performed poorly with resultant abnormal frenal attachments.
The patient and his family were counseled extensively regarding this. It was explained to them that his problem needed to be addressed at a specialty facial trauma care hospital. They were then referred to our hospital for treatment.
Anxiety of patient and his family allayed during initial consultation in our hospital
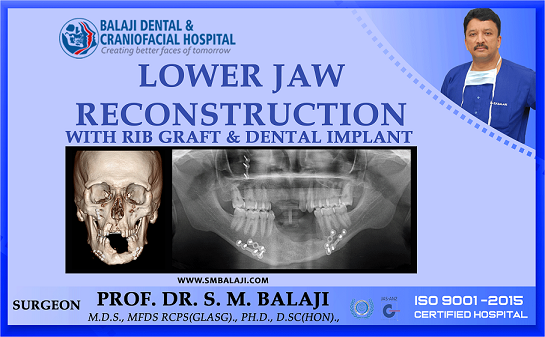
Dr SM Balaji, facial trauma care surgeon, examined the patient and ordered imaging studies including a 3D CT scan. There was malunion of the fracture along with reduced alveolar height. This had been caused due to the infection at the fracture site. There was also extensive loss of anterior teeth in both the maxilla and the mandible.
Treatment planning explained in detail to the patient and his family
It was explained that the patient’s infected titanium plates needed to be removed. This would be followed by reconstruction of the alveolar bone using bone grafts harvested from the patient. Nobel Biocare dental implants would then be placed for rehabilitation of the missing upper anterior teeth.
A period of six months would be allowed for bony consolidation of the graft to the alveolar bone. This would be followed by the placement of dental implants for rehabilitation of the missing lower anterior teeth.
Ceramic crowns would be placed on the dental implants following complete osseointegration of the implants to the surrounding alveolar bone. The patient and his parents were in complete agreement with the treatment plan and consented to surgery.
Successful completion of jaw reconstructive surgery for the patient
Under general anesthesia, an inframammary incision was made and a rib graft was harvested. A Valsalva maneuver was then performed to ensure that there was no perforation into the thoracic cavity.
Attention was turned to the maxilla where dental implants were placed in the anterior region. This was followed by a mandibular vestibular incision with the removal of the infected plates. The rib graft was then crafted to fit perfectly into the anterior alveolar defect. This was then fixed in place with screws and flaps closed with sutures.
Patient expresses understanding of postoperative instructions
The patient and his parents expressed their satisfaction with the treatment planning and the surgical results. They stated that they will return in six months for the complete rehabilitation of his oral structures.
Patient with lower facial asymmetry manifesting at birth
The patient is a 7-year-old female from Hastinapur in Uttar Pradesh, India. She had a minor degree of facial asymmetry at birth. This gradually worsened with age. It soon became apparent to her parents that there was an abnormality underlying her condition.
Worried over the turn of events, when she was around three years old, they had taken her to a local hospital.
Suspecting this to be the result of a genetic abnormality, they had been advised gene testing. Gene testing had revealed that the patient had the genetic abnormality linked to hemifacial microsomia.
Hemifacial microsomia explained to allay fears of the parents
The process causing hemifacial microsomia usually begins by the first trimester. It is still unclear as to the exact cause behind this condition. One probable cause could be disruption of vascularity to the face of the developing fetus. Though it usually manifests unilaterally, it can also occur bilaterally.
No external causes have been identified that lead to hemifacial microsomia. These include mother’s diet, metabolic conditions like diabetes or other such factors.
Parents were extensively counseled regarding the condition. It was explained to them that she had unilateral hemifacial microsomia, which involved her left lower face. There was also a minor deformity to the pinna of the left ear. They were informed that this would require cosmetic ear surgery at a later date.
Patients with hemifacial microsomia do not have prominent ears. Plastic surgeons perform ear reconstruction in most western countries.
The parents were advised that surgical correction of the deformities would be required for the patient at the appropriate ages. This would also include reconstruction of the affected side of the mandible.
Parents decide to seek consultation for correction of facial deformity
Deciding to get her condition corrected surgically, parents made widespread enquiries regarding the best surgeon to address this problem. They finally decided to come to our hospital for surgical management. Our hospital is a specialist craniofacial center with a dedicated craniofacial team.
Our hospital is a renowned center for facial asymmetry correction. Facial asymmetry arising from varied causes such as cancer, trauma and congenital causes are corrected surgically in our hospital. Facial reconstructive surgery is a specialty feature that has won accolades through our craniofacial program.
Initial presentation at our hospital for treatment of hemifacial microsomia
Dr SM Balaji, hemifacial microsomia surgery specialist, examined the patient and obtained comprehensive imaging studies including a 3D CT scan. This revealed that ramus and condyle were missing on the left side. There was no TMJ structure present. The patient had deviation of the mandible to the left side.
A comprehensive treatment plan was formulated and explained to the patient’s parents. It was explained that distraction osteogenesis cannot be performed due to insufficient bone. A costochondral rib graft with perichondrium would be harvested from the patient.
Harvesting with the perichondrium would enable lengthening of the ramus through growth as the patient grows up. In case growth of the ramus does not occur, ramus lengthening surgery through distraction osteogenesis would be performed.
The patient would also need TMJ reconstruction surgery at a later date. Parents expressed understanding of the treatment plan and consented to surgery.
Successful surgical placement of rib graft to posterior ramus
Under general anesthesia, an inframammary incision was made and a costochondral rib graft was harvested. This was followed by a Valsalva maneuver to ensure that there was no perforation of the thoracic cavity. The incision was then closed in layers with sutures.
Attention was next turned to the left ramus region of the mandible. An incision was made to expose the underdeveloped left ramus. The mandible was then pulled down and the costochondral graft with perichondrium affixed to the posterior ramus using titanium screws.
This resulted in improvement in facial symmetry for the patient. The wound was then closed with sutures.
It was explained to the parents that the patient would require further surgeries for complete rehabilitation of her facial deformity. Parents expressed understanding of the information and expressed their thankfulness before final discharge from the hospital.
Patient develops lower jaw swelling about a year ago
The patient is a 24-year-old male from Hoskote in Karnataka, India. He developed a swelling in the region of the left lower jaw around a year ago. This was especially alarming since he has always had asymmetry of the face with deviation of the mandible to the left side. The swelling was also associated with pain and subsequent tooth mobility in the involved region.
This had been followed by a visit to a local dental clinic where radiographic imaging had been obtained. A provisional diagnosis of odontogenic keratocyst had been made by the specialist there. It was explained to the patient that he needed to undergo left-sided partial mandibulectomy to resect the lesion. This would need to be followed by reconstruction of the jaw.
He had subsequently undergone surgery at a nearby city. The lesion had been resected, but unfortunately the condyle had been displaced superiorly into the region of the lateral pterygoid. This had resulted in worsening asymmetry of his face. The patient had become extremely distressed by this turn of events.
His parents had presented to the operating surgeon for a solution to his problem. Realizing the enormity of the condylar surgical correction and reconstruction required by the patient, the patient had been referred to our hospital for treatment.
What is an odontogenic keratocyst and how is it managed?
An odontogenic keratocyst is benign developmental cyst that is locally aggressive. Peak incidence is mostly during the second or third decades of life. At least 50% of odontogenic keratocysts are found in the posterior body and lower ramus of the mandible. Segmental mandibulectomy is performed, but results in gross residual deformities of the face.
Swelling is the most common presenting complaint. They may also be asymptomatic and found incidentally on dental radiographs. Plastic reconstructive surgery is necessary to full rehabilitate the patient. Usage of distraction devices helps restore facial symmetry. Implant treatment enables replacement of lost teeth.
Initial presentation at our hospital for treatment of his odontogenic keratocyst
Dr SM Balaji, jaw reconstruction surgeon, had examined the patient and obtained comprehensive imaging studies including a 3D CT scan. The 3D CT confirmed that the condyle had been superiorly displaced into the region of the lateral pterygoid muscle. He explained to the patient that he needed reconstruction of his resected jaw through bone grafts harvested from the patient.
He further explained that the patient’s idiopathic facial asymmetry could also be corrected through mandibular internal distractor surgery. A detailed explanation of the treatment process was given to the patient. Realizing that corrective jaw surgery would result in complete resolution of his facial asymmetry, the patient happily consented to undergo this surgery.
Successful mandibulectomy and internal distractor placement surgery
Under general anesthesia, the condyle was first brought back into correct anatomical position. This was followed by reconstruction of the resected mandible using the bone grafts. The bone grafts were fixed in position using titanium screws.
He also underwent placement of a left mandibular ramus distractor. A latency period of one week was allowed following placement of distractor. The distractor was subsequently activated by 1 mm each day for 18 days. This achieved an increase of 18 mm of mandibular distraction on the left side.
The time frame was explained to the family before surgery. It was explained that six months would be required for full consolidation of the new bone. He was instructed to return in six months. Distractor device would be removed and implants would be placed at that point. The patient expressed understanding of the instructions.
Patient returns for distractor removal surgery and dental implant surgery
A 3D CT scan was obtained at the site of distraction to check for bone consolidation. There was also good consolidation of the bone grafts at the site of the jaw reconstruction surgery. This was explained to the patient and he was scheduled for distractor removal and implant placement.
Removal of mandibular distractor and placement of dental implants
Under general anesthesia, an incision was placed in the left posterior region at the region of the distractor. A flap was then raised followed by removal of the left mandibular ramus distractor. Nobel Biocare dental implants were then placed in relation to the left mandibular second premolar and second molar. Hemostasis was achieved and wound closure was done using resorbable sutures.
Successful outcome of surgery with complete patient satisfaction
Complete symmetry of the patient’s face had been established through the distraction. The patient was extremely happy that he now had good facial harmony. He expressed how this would result in greatly increased social acceptance amongst peers. It was explained to him that he needed to return in three to four months for placement of ceramic crowns on the dental implants.
The patient expressed complete understanding of the instructions and expressed his happiness before discharge from the hospital.