TMJ injuries in childhood
Falls are common in childhood. However, a child’s bones are more flexible than adult bones and thus the chances of fractures are lesser than adults. Adult bones are denser and more mineralized that the bones of children.
However, there are certain injuries that are more common in children, which lead to complications. Injuries to the chin where there is direct impact from a fall can lead to injuries to the TMJ. When the impact is sufficiently high, this can lead to bleeding into the TMJ. In many instances, the child might not complain too much of pain in the TMJ. The parents might not be aware of the seriousness of the injury because of this and do not seek medical attention.
Consequences of injury manifesting with passage of time
It is only the passage of time that reveals the serious consequences that arise from this injury. The bleeding into the joint space results in bony fusion of the joints with the glenoid fossa leading to arrest in the growth of the lower jaw and difficulties with eating and speech.
Most cases of bony ankylosis of the mandible that arises in childhood could have been averted with timely medical help. It is therefore very important to seek medical help if such an injury occurs even if the child does not exhibit pain or too much discomfort in the period immediately after the fall.
The consequences of neglecting such an injury are high with the child needing to undergo multiple surgeries along with the psychosocial stress that arises from having facial deformity because of this.
Initial diagnosis of bilateral TMJ ankylosis and sleep apnea
This is a 7-year-old boy from Meghalaya in India who had first presented to Balaji Dental and Craniofacial Hospital in Chennai at the age of 5 with the chief complaint of a retruded mandible and displacement of the tongue to the back of the mouth. This boy had fallen down on his chin as an infant. This had been neglected by his parents at that time. Over time, his jaw growth stopped and he was unable to open his mouth to any degree. They had taken him to a facial plastic surgeon in his hometown. A plastic surgeon in India normally performs a wide variety of surgeries. He however informed them that he performed only cosmetic surgery and referred them here as our hospital is renowned for jaw correction surgery in India. Our hospital rigorously follows the protocols laid down by the American Association of Oral and Maxillofacial Surgeons.
Dr SM Balaji, jaw reconstruction surgeon, examined the patient and obtained a detailed history from the parents. His parents said that the boy periodically stopped breathing during sleep and resumed his breathing with a loud gasp. The patient was diagnosed with bilateral TMJ ankylosis and sleep apnea resulting from backward placement of the tongue due to the micrognathia.
Need for multistage surgical correction explained to the patient
Sleep apnea is a potentially serious sleep disorder in which breathing repeatedly stops and restarts. It was explained to them that surgery needed to be done in two steps for complete correction of the patient’s problems. Orthognathic surgery or sleep apnea correction surgery was performed first as it had to be corrected first. Release of the bilateral TMJ ankylosis would be performed at a later date. A tracheostomy had to be performed due to his restricted mouth opening following which bilateral mandibular body distraction osteogenesis surgery corrected his micrognathia. Bone grafts would not be needed taking into account the age of the patient.
Parents present with patient for TMJ ankylosis surgery
The patient presented with his parents now for corrective jaw surgery for release of his bilaterally ankylosed TMJ. He still has difficulty eating as he was still unable to open his mouth. His parents stated that he has been on a predominantly liquid diet and has lost quite a bit of weight because of this.
Presurgical diagnostics and treatment plan for the patient
Dr SM Balaji examined the patient and ordered comprehensive imaging studies. The patient’s 3D CT revealed that there was complete bony ankylosis between the mandibular condyle and glenoid fossa. His mouth opening was zero due to bilateral TMJ ankylosis. It was decided to perform a tracheostomy as intubation would not be possible due to nil mouth opening. TMJ ankylosis surgery would be performed following the tracheostomy.
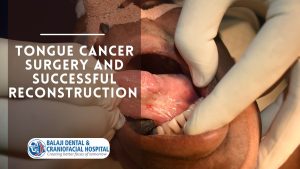
Surgical release of the bilateral TMJ ankylosis
Under general anesthesia, a horizontal skin incision was first made through the previous tracheostomy scar. Minimal dissection was carried out and the strap muscles were retracted. A tracheal incision was made and maturation sutures placed. A tracheostomy tube was then inserted following which skin closure was done in layers.
Attention was then turned to the bilaterally ankylosed temporomandibular joints. An incision was first made in the submandibular region bilaterally and dissection was performed down to the temporomandibular joint. The ankylosed bone was osteotomized bilaterally and gap arthroplasty was performed. Following excision of the bony mass, mouth opening was achieved passively to about 35-40 mm. The incisions were then closed using sutures.
Postsurgical care for the patient
Mouth opening of about 3.5 mm was achieved at the time of surgery. Physiotherapy was initiated for the patient after surgery with jaw exercises under supervision. Mouth opening exercises were also performed for about a month with regular follow up.
The parents were very happy and satisfied with the results. They expressed their delight that he was able to eat normal food without any restrictions now and has slowly begun to gain weight since then. They were instructed to return after six months for a final checkup at the hospital